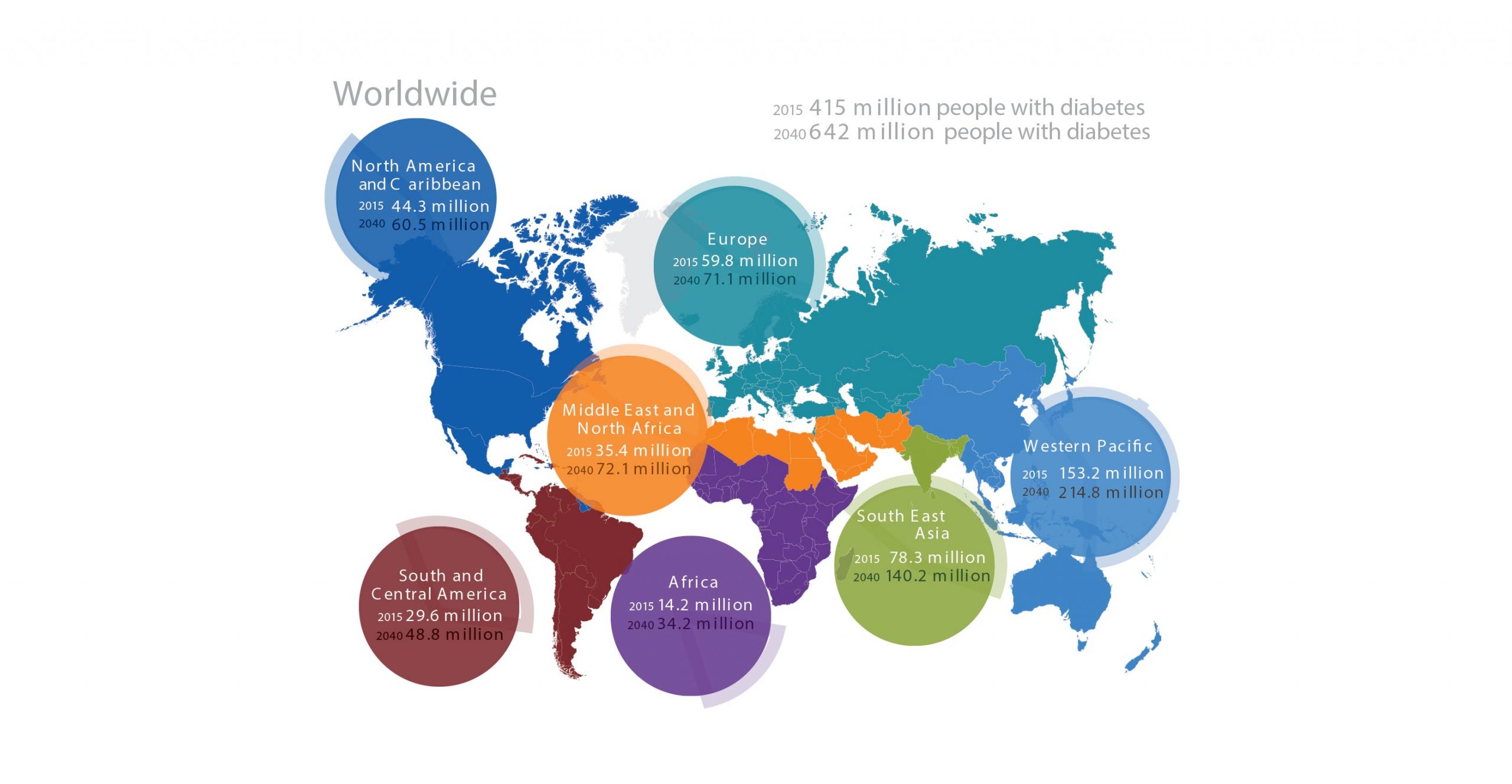

The International Diabetes Federation (IDF) has included Bangladesh as one of the countries in their South-East Asia (SEA) region. Of the 415 million people inflicted with diabetes of which 78 million are within the SEA region.
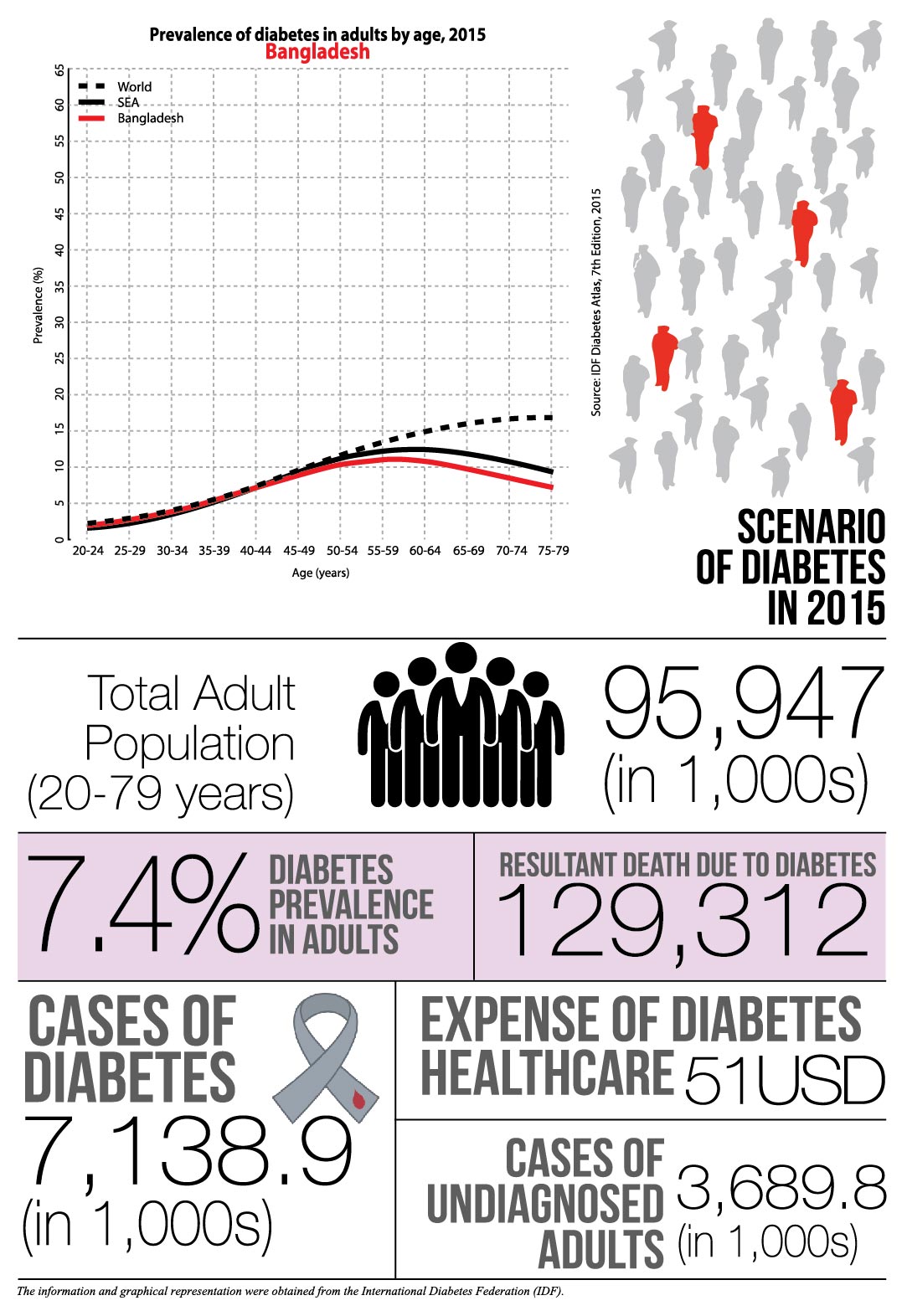
The IDF has inferred that there will be 140 million cases in the region by 2040. As of 2015, there were 7.1 million cases in Bangladesh. The prevalence of diabetes is only predicted to increase significantly within the coming year.
This is evident when comparing the disease trend in 2013 to that of the previous year. During 2013, the prevalence of diabetes was 5.52%, an increase of 34% in 2015, and the undiagnosed population was 2,218.82. There were total 5,089,040 cases with 102,139 deaths related to the disease; the cases have increase by 40% in merely 2 years. The expenditure was for healthcare was $10 less as $41.
“Our association has grown from a singular entity to 99 centers, treating approximately a 30% of the diabetic population. We aspire to treat 50% of the population by 2020.”
– Professor Azad Khan
Professor Azad Khan is the President of the Diabetic Association of Bangladesh.
Could you elaborate on the state of diabetic prevalence, healthcare and awareness of Bangladesh in a global context?
The world is passing through an epidemic of Type 2 diabetes and the lesser-known gestational diabetes (GDM). The general population is unaware that epidemic such as this produces a greater effect on developing countries such as ours. For example, diabetes is increasing at a faster rate in Bangladesh than Northern Europe. There are some reasons for this, but the predominant cause is the lifestyle changes within our nations. Developed countries have already established their dynamic, and we are trying to reach that point. Our rapid urbanization has resulted in a decline of physical activities, increased fast food consumption, and obesity.
In LDCs such as Bangladesh, there is a focus on communicable diseases. Why should there be a greater shift towards a focus on non-communicable diseases such as diabetes?
Diabetes is one of many non-communicable diseases, which currently accounts for more deaths than communicable diseases. The major factor is that communicable diseases are episodic in nature meaning that they are cured after a period of time. On the other hand, non-communicable diseases need a lifetime management. Communicable diseases have come into control as a result of immunization and improved sanitary conditions.
What improvements need to be made in clinics, healthcare professionals and treatment methods in Bangladesh?
With communicable diseases, it is about creating a lifetime treatment plan. In our country, there are many hospitals but without provision of health education or follow-up system, components that are essential for the treatment of diabetes. We need a system of health education for these disease states; a diabetic patient is not given the same dosage of insulin throughout the entirety of their lives, it must be adjusted accordingly, and the patients and their families need to be educated on this. Furthermore, the doctor should advise the person on their dietary requirements, exercise and lifestyle practices to control their blood sugar.
 BADAS has profoundly contributed to the awareness and treatment of diabetes. Could you elaborate upon this accomplishment?
BADAS has profoundly contributed to the awareness and treatment of diabetes. Could you elaborate upon this accomplishment?
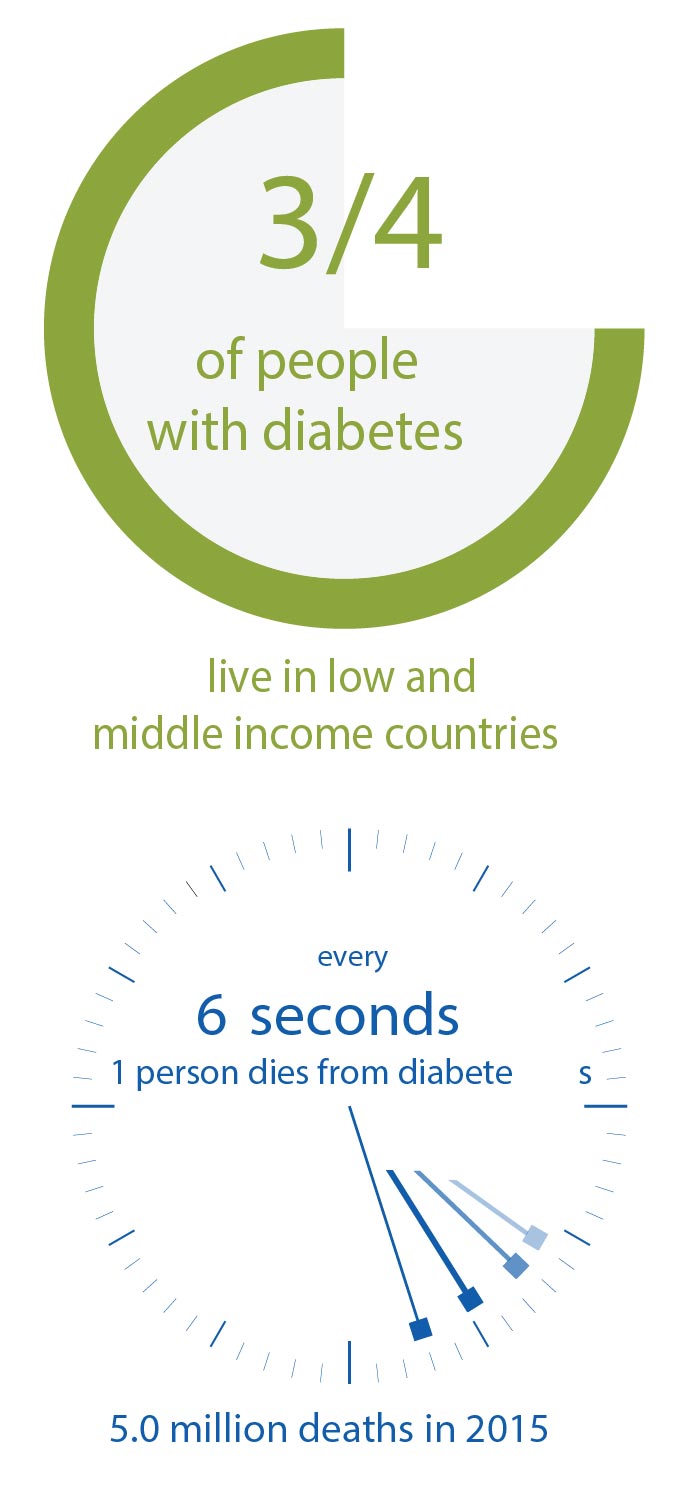
Our association has grown from a singular entity to 99 centers, treating approximately a 30% of the diabetic population. We aspire to treat 50% of the population by 2020. Our vision is to raise the accessibility, affordability and awareness of the disease throughout the nation to prevent the predicted rate of prevalence. The stark reality if that only 20 percent of the expenditure for diabetes were from low and middle-income countries where 80 percent of the diabetic population resides. When we look at the context of Bangladesh there is only one physician for every 3,400 citizens; roughly half of these doctors are taught elementary information regarding diabetes and a quarter are taught management of diabetes.
How has the partnership between Novo Nordisk and BADAS changed the perspective of diabetes in Bangladesh? What projects have you planned for the future?
Our partnership has allowed for the consistent supply of insulin and the emergence of many diabetes-related programs. Insulin was not usually available below district head quarters. We took the initiative to train at least one physician at the Upazila headquarters and equip their chambers with a fridge and other gadgets needed for primary diabetes care center with the financial assistance from the Novo Nordisk. These DLP trained physicians have started to make insulin available at the Upazila levels. We are working on a plan with the local imams, teaching them how to measure blood glucose and raise awareness. They have a significant degree of influence, and this allows them to raise awareness to a broad audience.
How is DLP training of physicians improving the care of diabetes? What significant outcomes have you witnessed?
Through DLP we have been able to train over 10,000 GPs. Matrix International, a Harvard-based research group, evaluated the impact. The findings show that DLP has improved all aspects of diabetes care including prevention and care of Gestational Diabetes Mellitus
( GDM).
Given that we are a nation with such a flourishing pharmaceutical industry, what are the challenges in obtaining insulin at a lesser cost? Are there any other alternative medications or regimes that would be more feasible for the nation?
The best option to reduce cost is the robust primary prevention program. We have submitted a draft to the Govt. for adopting a National Prevention Programme. The main emphasis is to create awareness for health life style. Secondary and tertiary preventions are also necessary so that diabetics do not develop complications, which increase costs enormously. Locally produced medications should be cheaper, but drug control authorities should develop the capacity to monitor quality and implement quality control.
“The total annual per capita expenditure on medical care was 6.1 times higher for diabetes than non-diabetes (USD 635 vs. 104, respectively).”
– Dr. Shariful Islam
Dr. Shariful Islam is a postdoctoral research fellow and scientist at Cardiovascular Division, The George Institute for Global Health and affiliated with the Sydney Medical School, University of Sydney. He is also a faculty and principal investigator at the Non-Communicable Diseases Unit, International Center for Diarrheal Disease Research, Bangladesh (ICDDR, B). He has received several national and international awards, including a gold medal for academic excellence, Fogarty Fellowship, Packard Award and DAAD Fellowship.
Though eHealth is an expensive method to initiate, it will change the dynamic of disease state management. How will it improve the scenario of diabetes management in Bangladesh?
In recent years, eHealth has been shown to improve disease management in both the developed and developing countries. In a randomized controlled trial of 240 patients in Dhaka (published in Diabetes Care in 2015), we demonstrated that mobile phone text messaging could improve diabetes management in a low-income country like Bangladesh. Text messaging has been a low-cost, simple intervention to inform, motivate and improve the risk factors for several chronic diseases. In another study, we reported that patients with diabetes in Bangladesh are willing to pay a small amount of fee to receive mobile phone diabetes services. With increasing access to cell phones and chronic diseases, this can be a sustainable method to provide additional service to patients in countries like Bangladesh.
The cases of diabetes in Bangladesh are becoming more prevalent with a predicted increase of 50% by 2030. How can the local population prevent this growth?
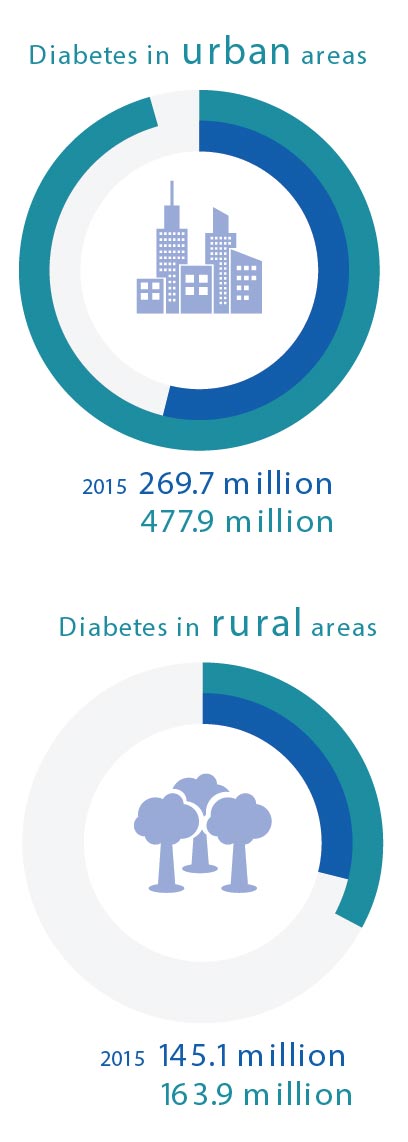
Prevention is the key to reducing diabetes and other chronic disease epidemics. With the increase in aging population, urban migration, unhealthily diet and sedentary lifestyle, the prevalence of diabetes are expected to increase several folds in the coming years. We reported the increasing prevalence of diabetes in both urban and rural areas in Bangladesh. There is a need to adopt both population-based and individual-risk-based approaches as well as primary and secondary prevention policies. Policies need to target creating greater awareness for local people using culturally appropriate media for healthy diet and lifestyle.
 Could you elaborate upon the common perceptions of diabetes in the country? How do education and income impose as factors in this scenario?
Could you elaborate upon the common perceptions of diabetes in the country? How do education and income impose as factors in this scenario?
In a recent study, we reported that patients with type 2 diabetes in Bangladesh have limited knowledge on the causes, management and risk factors for diabetes, despite receiving professional health education and care in a tertiary diabetic hospital. Strategies to improve the quality of diabetes education and identifying other potential factors for glycemic control are essential for ensuring optimum management of diabetes in Bangladesh. There is a need to increase health education about prevention of diabetes and its consequences. Although diabetes was thought to be a disease of the rich people, it is now proven that diabetes impacts the lives of both poor and rich people.
According to your study, the prevalence of diabetes ranges from 4.5% to 35% in various parts of Bangladesh. What are primary factors that contribute to the areas with the highest prevalence?
In a recent systematic review of the risk factors for diabetes in Bangladesh, we identified 14 common risk factors for diabetes in Bangladesh, namely increased age, obesity, waist-hip ratio, social class, hypertension, family history, sedentary life style among others. The potential risk factors differed by urban-rural areas and by gender. Several risk factors contribute to the increasing prevalence of type 2 diabetes. Our reviews suggest “metabolically-disadvantageous” body composition of more abdominal and visceral fat in Bangladeshi adults might cause higher diabetes risk at a lower BMI compared to the Western populations. Preventive strategies targeting to control risk factors for diabetes is a priority public health issue and should be considered for early intervention by clinicians and policy makers.
The total cost for medical care and medication for diabetic patients is significantly higher in Bangladesh. Why are treatment and medication that much more expensive within the nation?
We analyzed the healthcare use and expenditure for diabetes in Bangladesh in a case-control study among 1,200 patients (BMJ Global Health 2016, In Press). Our study showed that participants with diabetes had two times more days of inpatient treatment, 1.3 times more outpatient visits, and 9.7 times more medications than non-diabetes participants (all p<0.005). The total annual per capita expenditure on medical care was 6.1 times higher for diabetes than non-diabetes ($635 vs. 104, respectively). Using the IDF estimates of 8.4 million diabetics in Bangladesh, the total estimated healthcare expenditure for diabetes in Bangladesh is around $5.3 billion. The high costs might be attributed to increased costs of medication and hospitalization. Although medicines are comparatively cheaper in Bangladesh, we found that patients are often prescribed more expensive medications with similar clinical effects when more affordable options are available. Also, patients are often suggested unnecessary tests and hospitalization which might increase the costs.
How should multi-sectoral approaches and cost-effective prevention strategies be implemented in Bangladesh?
The multi-sectoral approach should be led by the Government with support from different stakeholders. The Government should identify cost-effective prevention strategies using evidence-based approaches and pilot studies.
What are the multi-fold cost implications of diabetes?
Diabetes is a costly condition and can lead to several disabling and life-threatening complications, including stroke, heart attack, chronic kidney diseases, neuropathy, visual impairment, and amputations. Studies in Bangladesh reported eye problems, chronic kidney diseases, cardiovascular diseases, and depression as major complications. Although most of these complications can largely be prevented through the use of several inexpensive, easy-to-use and cost-effective interventions, the utilization of these interventions in developing countries, where the majority of persons with diabetes live, remains tragically low. It is estimated that healthcare expenditure for diabetes accounts for 10.8% of the total annual healthcare expenditure worldwide, which totaled at least $548 billion in 2013 and is projected to exceed $627 billion by 2035. The social and economic impact of diabetes is complex and difficult to measure. The costs of human suffering, loss of income and pleasure of life, low quality of life and other sufferings cannot be measured in monetary units alone.
Information, facts and figures are provided by the International Diabetes Federation.
The interviewee can be reached at shariful.islam@icddrb.org. His publications can by found at
www.researchgate.net/ profile/Sheikh_Mohammed_ Shariful_Islam